Critique 303 – Association between alcohol consumption and breast cancer incidence and prognosis: A systematic review and meta-analysis
Arecco, L., Cacilhas, P.M., Bobato Lara Gismondi, C., Bruzzone, M., Gentile, G., Gerosa, R., Blondeaux, E., Agostinetto, E., Dauccia, C., Lobo-Martins, S., Grochot, R., Saini, K., Azim Jr., H.A., Debiasi, M., De Caluwé, A., Buisseret, L., Del Mastro, L., Lambertini, M., de Azambuja, E.
The Breast 86 (2026) 104719. https://doi.org/10.1016/j.breast.2026.104719
Abstract
Background: While alcohol consumption appears to influence the incidence of breast cancer (BC), its association with prognosis after a BC diagnosis remains less established. This meta-analysis aimed to explore the association between alcohol consumption on both BC incidence and outcomes.
Methods: A systematic literature search was conducted up to May 1st, 2025 (CRD42025593784). Retrospective and prospective studies reporting BC incidence, recurrences, and survival outcomes in women with history of alcohol consumption were included. Analyses according to alcohol intake levels (light, intermediate, heavy consumption) were performed. Main outcomes were BC incidence, BC recurrences, BC-specific survival (BCSS), and overall survival (OS). Pooled relative risk (RR) and hazard ratio (HR) with 95% confidence interval (CI) were calculated.
Results: Out of 5208 screened records, 37 studies including 2,565,920 women were included. Among 17 studies reporting on BC incidence, any alcohol consumption was associated with an increased BC incidence (RR 1.17, 95%CI 1.09–1.26; p < 0.001). BC incidence increased proportionally with higher levels of alcohol consumption: light RR 1.13 (95%CI 1.05–1.23; p = 0.002), intermediate RR 1.28 (95%CI 1.18–1.39; p < 0.001), and heavy consumption RR 1.52 (95%CI 1.38–1.67; p < 0.001). Among 20 studies assessing BC outcomes, no associations were found between alcohol consumption and BC recurrences (RR 1.02, 95%CI 0.93–1.11) nor BCSS (HR 0.93, 95%CI 0.87–1.00), while light and intermediate alcohol consumption were associated with slightly improved OS: HR 0.85 (95%CI 0.78–0.92; p < 0.001) and HR 0.84 (95%CI 0.75–0.94; p = 0.002), respectively.
Conclusions: Among over 2.5 million women, alcohol consumption was associated with a dose-dependent increased risk of BC, while alcohol consumption did not appear to worsen prognosis in patients with prior BC diagnosis.
ISFAR Summary
Arecco et al. (2026) provide a comprehensive synthesis of the relationship between alcohol consumption and breast cancer incidence and prognosis, drawing on data from over 2.5 million women across 37 studies. Although a statistically significant association is reported, the magnitude of the observed effect is weak from an epidemiological standpoint. A large degree of heterogeneity is also reported, indicating that this association is highly susceptible to residual bias and uncontrolled confounding, thus limiting causal inference.
Arecco et al. (2026) report a relatively high increase in risk with alcohol consumption, namely 13-28%, whereas other meta-analyses report lower increases. These differences will most likely be determined by the studies included in the analysis, with assessments of alcohol consumption varying across them, recall bias leading to underreporting, and other biases, such as a lack of information on drinking patterns, as well as the role of other socioeconomic and lifestyle factors. Differences may also be determined by excluding some studies that did not find an association between alcohol consumption and breast cancer risk.
The study’s clinical significance lies in its finding that alcohol appears to have a limited effect on breast cancer prognosis. In addition, no significant association was observed with recurrence or breast cancer–specific survival, whereas a significant beneficial association was observed with overall survival. While the study strengthens the existing evidence for alcohol reduction in cancer prevention, this new evidence on survivorship and prognosis should be interpreted cautiously.
Background
Breast cancer (BC) is the most common type of cancer in women, and the first purported positive association between alcohol consumption and breast cancer was reported in 1977 (Williams and Horm 1977). Although treatment has advanced and is now relatively successful, BC remains the second leading cause of cancer death in women after lung cancer (American Cancer Society, 2026). Therefore, regularly updating and reviewing the latest literature is important.
BC has many risk factors; several of these are not modifiable. Non-modifiable risk factors include getting older, specific genetic mutations, early menstrual periods, late or no pregnancy, starting menopause after the age of 55, having dense breasts, personal and family history of breast cancer, and previous radiotherapy (Debela et al., 2025). Modifiable risk factors include lack of physical activity, being overweight or obese after menopause, using hormone therapy, taking oral contraceptives, and alcohol consumption (Jung et al. 2016, Francies et al. 2020). Since BC is a common type of cancer and the risk may be influenced to some extent by lifestyle factors such as alcohol consumption, considerable attention is given to the relationship between BC and alcohol consumption.
Consuming alcohol has been dose-dependently associated with an increased risk of BC. The impact of alcohol consumption on BC risk varies between studies; some report an increase of approximately 4% per daily glass of alcohol (Seitz et al., 2012) whereas others have reported an increase of approximately 10% per daily glass of alcohol (U.S. Surgeon General., 2025). These estimated risk increases are relative risks. So, one should understand that, because one in eight women will develop BC, women have an overall risk of 12.5%. Drinking one glass of alcohol daily will increase that risk from 12.5% to [12.5 + (4% x 12.5) or 12.5 + (10% x 12.5)], which is 13 or 13.75%.
Previous ISFAR critiques (ISFAR #285, #270, #265 and #241, for example) also addressed systematic reviews and meta-analyses of BC incidence. Arecco et al. (2026) address not only the relationship between alcohol consumption and BC incidence but also BC recurrence and overall survival, which have been less addressed in studies. The authors selected papers published after 2000, yielding two sets of studies: one focusing on BC incidence and another on BC recurrence and overall survival. The incidence analysis included 2,450,932 women, and among these, 53,465 women with a history of alcohol consumption were subsequently diagnosed with BC. The conclusions drawn were essentially similar to those reported before: alcohol consumption, even moderate drinking, increases the incidence of BC, and alcohol consumption does not affect BC recurrence and is actually linked to a slightly improved overall survival.
Critique
While meta-analysis by Arecco et al. (2026) confirms and reinforces previous results, it is striking how the relative risks vary across meta-analyses. As indicated above, the relative risk ranges from approximately 4% to 10% per daily glass of alcohol. Arecco et al. (2026) report a 13% increase for the light alcohol consumption group compared with non-consumption, which is defined as the group drinking up to one glass of (10 g) alcohol per day. The intermediate group, defined as > 10 g alcohol and < 20 g of alcohol per day, has an increased risk of 28%, which is relatively high compared to some other previous meta-analyses and systematic reviews. Such differences will most likely be determined by the studies included in the analysis, with assessments of alcohol consumption varying across them, recall bias leading to underreporting, and other biases, such as the lack of information on drinking patterns, as well as the strong correlation between alcohol consumption and socioeconomic and lifestyle factors that may independently influence cancer risk and survival.
Arecco et al. (2026) also reported the incidence of BC by tumour subtype (i.e., hormone receptor status). Alcohol consumption appeared to be associated with a higher risk of hormone-receptor-positive BC, while no significant association was found between alcohol consumption and the incidence of hormone-negative BC. Since a large proportion of BC cases involve hormone receptor-positive tumours (70-80% of all BC cases), this first key finding supports the idea that hormonal pathways, especially those related to oestrogen, are central to the biological connection between alcohol and breast cancer, and could explain why the effect of alcohol varies across different breast cancer subtypes (Al-Sader et al., 2009). It is well documented that there is a positive association between the risk of development of breast cancer and the concentration of steroid hormones for both pre- and post-menopausal women; the steroid hormones include androgens, such as testosterone, and estrogens, such as estradiol, estrone and estriol (Kaaks et al. 2005a,b). One source of endogenous estrogens is the aromatisation of androgens to estrogens, and alcohol has been observed to increase this aromatisation; the conversion occurs primarily in the ovary for pre-menopausal women and peripherally for post-menopausal women. The authors thus suggest that, although a causal relationship cannot be definitively established, reducing alcohol consumption remains an important modifiable risk factor for BC prevention.
A second aim of Arecco et al. (2026) was to examine the effect of alcohol consumption on BC recurrence, breast cancer-specific survival and overall survival. Interestingly, neither parameter is negatively affected by alcohol consumption. However, as the authors highlight, alcohol consumption is often measured prior to diagnosis rather than afterwards, and there is limited monitoring of changes in drinking behaviour after treatment, which is a major limitation of existing studies.
A potential biological explanation for this lack of association between BC recurrence and alcohol consumption is that the processes that trigger cancer (carcinogenesis) are not always the same as those that promote tumour growth or recurrence (Murray, 2015). The initiation of the tumour is linked to alcohol, with acetaldehyde, the primary metabolite of alcohol, directly damaging DNA and impeding repair mechanisms, leading to mutations that can result in the development of the first cancer. The promotion of the existing tumour, however, may be less closely linked to alcohol, as once a tumour is established, its recurrence depends more on the tumour’s inherent aggressiveness, systemic inflammation, or hormonal factors, which may not be significantly influenced by low levels of alcohol. Furthermore, although alcohol is known to raise oestrogen levels, which can promote oestrogen receptor-positive (ER+) cancers (Al-Sader et al., 2009), many patients receive anti-oestrogen treatments such as tamoxifen or aromatase inhibitors after diagnosis. These adjuvant therapies effectively block the estrogen-increasing effects of alcohol, neutralising the pathway that would otherwise promote recurrence.
It has also been suggested that while low levels of the enzyme aldehyde dehydrogenase in breast tissue, which detoxifies acetaldehyde, increase the breast’s vulnerability to initiation by alcohol, in an already treated patient, the amount of acetaldehyde produced by moderate drinking might not reach a sufficiently high concentration to promote new growth in any dormant cancer cells. Additionally, after radiation and chemotherapy, any remaining dormant cells might have a different metabolic profile, rendering them less vulnerable to the specific DNA damage caused by acetaldehyde (Brooks and Zakhari 2015)
Another possible explanation is changes in drinking habits after a first BC incident. This is, however, not likely since recurrence was studied in women who drank alcohol after their first incidence of breast cancer. Alternatively, methodological aspects or unknown confounders, such as cancer screening (Mu and Mukamal, 2016), may still be relevant for the alcohol–breast cancer association but are currently missing from the overall picture.
The third key finding of ‘slightly’ improved overall survival in women who had already been diagnosed with light and intermediate alcohol consumption may, as the authors suggest, be due to beneficial effects on other conditions, such as cardiovascular disease events or residual confounding. Interestingly, the hazard ratios reported for this finding were 0.85 and 0.84 for light and intermediate alcohol consumption, respectively, corresponding to reductions of 14% or 15% in overall survival. Conversely, a 13% and 28% increased risk for an initial BC incidence was seen as a key reason to advocate limiting alcohol consumption to reduce cancer risk.
It is interesting to see how positive and negative relative risks are interpreted differently. The relationship between alcohol consumption and BC risk is very complex and should be recognised as present but not as a proven fact to justify restrictive measures for alcohol consumption.
In conclusion, this systematic review and meta-analysis by Arecco et al. (2026) provides a comprehensive and methodologically rigorous synthesis of the relationship between alcohol consumption and breast cancer incidence and prognosis, drawing on over 2.5 million women across 37 studies. The findings confirm alcohol consumption as a modifiable risk factor, particularly for estrogen receptor-positive breast cancer, with risk increasing in a dose-dependent manner. However, the study’s clinical significance lies in its finding that alcohol appears to have a limited influence on breast cancer prognosis, as no significant association was observed with recurrence or breast cancer–specific survival, even among heavy drinkers. Importantly, this absence of association should not be interpreted as evidence of safety, as limitations in self-reported exposure measurement, inadequate assessment of post-diagnosis drinking behaviours, and residual confounding may obscure a true relationship. Accordingly, while the study strengthens the evidence for alcohol reduction in cancer prevention, its implications for survivorship and prognosis remain uncertain and should be interpreted with caution.
Specific Comments
Forum Member Skovenborg states that “alcohol is classified as a group 1 carcinogen “alongside tobacco and asbestos”. As of March 2026, there are over 135 agents, mixtures, and exposure circumstances listed in Group 1, including, for example, tamoxifen (an anti-oestrogen drug), diesel exhaust, wood dust, processed meat, and Chinese-style salted fish. Full-text articles reporting no association between alcohol and breast cancer were excluded according to the flow diagram. If you are studying the possible association between alcohol consumption and breast cancer how is it OK to exclude studies with a “no association” result? And how would the relative risk calculations look if these studies were included? Is this decision introducing an information bias?
Light alcohol intake (≤ 10 g/day) is a fictional figure, calculated by dividing most data on weekly alcohol intake by 7. There is a risk difference between drinking 70 grams of alcohol over the weekend and taking 10 g a day with a meal.
Significant heterogeneity was observed across the included studies. Given this serious problem, why should the results not be interpreted with “extreme caution”? A recent Norwegian review of risk factors for breast cancer reached the following conclusion: “It is surprising that alcohol consumption was not in the “top list” of risk or causes of breast cancer, since alcohol consumption is listed as a risk factor, and deaths from breast cancer are linked to alcohol use (Løyland et al. 2024). Three systematic reviews of alcohol use and breast cancer are included in this evidence synthesis, two with meta-analyses, and it is interesting to note that the findings are inconsistent. The conclusions varied from “there is an association” between alcohol consumption and breast cancer risk, to “the association remains insufficient”, to “high intake of wine contributes” to breast cancer risk, but “protection is exerted with low doses of wine”. Although one of these meta-analyses concluded with an association with an effect size of 1.28, the result did not qualify for our “top list” because of high heterogeneity (I2 = 73.5%). In addition, in the systematic review without a meta-analysis, researchers found a positive association in one study, while another study showed a nonsignificant inverse association. The authors of this systematic review reported low methodological quality and a small number of included studies.”
Forum member Ellison “Agrees with the initial comments of other Forum members, as stated in the Critique, that this is a very well-done analysis and publication that supports the potential adverse effects of alcohol consumption on the occurrence and recurrence of breast cancer. This and earlier studies suggest that the increase in breast cancer risk among light drinkers is modest, but risk rises among women who drink heavily. Further, little effect of alcohol intake is observed on breast cancer recurrence or death from breast cancer. However, among women with breast cancer, a beneficial effect of alcohol consumption on total mortality is notable, with about a 15% decrease in risk for light and moderate drinkers. We assume that the protective effects of moderate drinking on cardiovascular risk underlie these findings.
The initial results reported in this paper concern the relationship between total alcohol intake and breast cancer risk. Given that the association between alcohol and disease is non-linear, these data are less informative than those demonstrating risk at varying levels of consumption.
To what extent can these data provide advice for an individual woman? Since the effects of alcohol consumption are markedly affected by cultural and lifestyle factors (including education, income, dietary factors, smoking habits, obesity, and especially the pattern of drinking), the results of these analyses are limited in providing the data needed to develop drinking advice for an individual woman. For this, data are needed on the effects among women in similar socio-economic and cultural settings and with similar patterns of drinking. One possible avenue to explore this might be to evaluate a woman’s frequency of mammography. This seems to be affected by lifestyle factors, with more frequent mammography among those with higher socio-economic status, and thus presumably a higher chance of identifying early cancers. As such, women who tend to drink more might be found to have a higher alcohol-related cancer risk.“
Forum member Romano considers that “The relationship between alcohol consumption and breast cancer, as presented in this meta-analysis, must be interpreted with caution because of important methodological limitations that compromise the causal validity of the findings. Although a statistically significant association is reported, the magnitude of the observed effect (RR 1.17) is weak from an epidemiological standpoint and falls within a range highly susceptible to residual bias and uncontrolled confounding, thereby limiting causal inference.
A central concern is residual confounding. Alcohol consumption is closely associated with socioeconomic, behavioural, and biological variables, including socioeconomic status, diet, body mass index, physical activity, reproductive history, and hormonal therapy use. These factors are inconsistently controlled for across studies, and the ‘healthy moderate drinker’ effect introduces systematic bias, as moderate drinkers often have better overall health profiles and greater access to healthcare.
The extreme heterogeneity across studies (I² = 92%) further undermines interpretability. The pooled estimate combines heterogeneous populations, study designs, and exposure definitions, limiting both internal coherence and external validity. Measurement of alcohol exposure is another major limitation. Most studies rely on self-reported intake, with inconsistencies in timing, quantification, and categorisation. Harmonising into standardised exposure groups introduces misclassification bias, which may attenuate or distort associations.
Although biological mechanisms support a potential carcinogenic role for alcohol, including acetaldehyde-mediated DNA damage, oxidative stress, and hormonal modulation, the modest magnitude of the observed associations raises concerns about bias.
The finding of improved overall survival among moderate drinkers is particularly problematic. This observation lacks biological plausibility and is likely explained by systematic biases, such as the ‘healthy drinker bias’ and ‘sick quitter bias’, in which non-drinkers may include individuals with pre-existing illness.
From a sampling perspective, aggregating heterogeneous study designs across diverse populations and time periods limits comparability and generalisability. Selection bias is also likely, as several cohorts involve specific subpopulations.
Finally, the definition of the reference group is a critical limitation. Including both lifelong abstainers and former drinkers introduces bias that may distort estimates of incidence and survival. Overall, although the study suggests an association between alcohol consumption and breast cancer risk, methodological limitations preclude strong causal conclusions. Prognostic findings should be interpreted with caution, as they are likely influenced by bias rather than by true biological effects.”
Forum member Harding considers that “the rationale for this paper is set out in the Introduction. The first paragraph identifies alcohol consumption as a modifiable risk factor that may influence breast cancer incidence, citing references 4 and 5. Reference 4 (Harborg) concerns obesity and does not mention alcohol at all. Reference 5 (Islami) lists alcohol consumption as one of 18 modifiable risk factors attributed to all cancer cases in the USA, but makes no claims about causation.
2. The second paragraph of the Introduction simply states that alcohol intake is a well-established modifiable risk factor for cancer and cites Reference 6 (Rumgay). The authors of this paper work for the International Agency for Research on Cancer and state that alcohol consumption was causally related to breast cancer in IARC Monographs published in 2010 and 2012.
3. The 2010 Monograph was No. 96, devoted to Alcohol Consumption and Ethyl Carbamate. Paragraph (f) in the Preamble (p. 19) concerns the Criteria for Causality. It states that the Working Group makes a judgment on the strength of evidence that the agent in question is carcinogenic in humans. It further states that, in making this judgement, the Working Group considers the Bradford Hill criteria, but there is no account of how the criteria are applied in particular cases, i.e. the process is not transparent. On page 13, it states that the IARC Working Groups strive to achieve a ‘consensus evaluation’. Consensus reflects broad agreement among Working Group Members, but not necessarily unanimity. The conclusion that malignant tumours of the female breast are causally related to the consumption of alcoholic beverages (6.1, p. 1278) is a result of this process, but the rationale for the conclusion is not explained and is not known. There are no criteria mentioned that need to be met before the evidence is ‘sufficient’ to conclude that alcohol causes breast cancer. In paragraph 6(e) on page 33, it states that the reasoning the Working Group used to reach its evaluation is presented and discussed, but where is it?
4. The 2012 Monograph was No.100E, on Personal Habits and Indoor Combustions. It simply cited the conclusions of the 2010 Monograph but also included more recent studies. Several studies showed negative associations, but the conclusion was again that alcohol consumption is causally associated with cancer of the female breast.
5. The Introduction goes on to assert that ‘Recent evaluations have reaffirmed the link between alcohol and breast cancer incidence, estimating that women who consume two alcoholic drinks per day have a 10-20% higher risk of developing breast cancer compared to non-drinkers’. The reference cited is the 2025 US Surgeon General’s Advisory on Alcohol and Cancer Risk, which cites two papers in support of this position (Sarich et al and Jung et al). Both papers find positive associations between alcohol consumption and breast cancer, yet again gloss over the crucial difference between association and causation.
6. The US Surgeon’s General Advisory does acknowledge, on page 7, that ‘Determining whether there is a causal relationship between a risk factor and a health outcome such as cancer is done through comprehensive assessments of scientific evidence and the application of well-established scientific criteria such as the Bradford-Hill criteria’, but then makes absolutely no attempt to do so.
7. So let’s apply some of them now. The first is Strength of the association. The increase in breast cancer rates reported in these papers is about 10% per additional drink per day. Reading Bradford-Hill’s original paper, it is clear that he would regard that as a very small effect. Another is Plausibility. Certainly, there are mechanisms by which alcohol consumption could lead to cancer, but where is the evidence that any of them actually causes breast cancer, especially when the cause of breast cancer is unknown? A third is Consistency. Has it been repeatedly observed by different people, in different places, circumstances and times? There is no shortage of studies on alcohol consumption and breast cancer. A graph taken from Sohi et al illustrates the general picture:
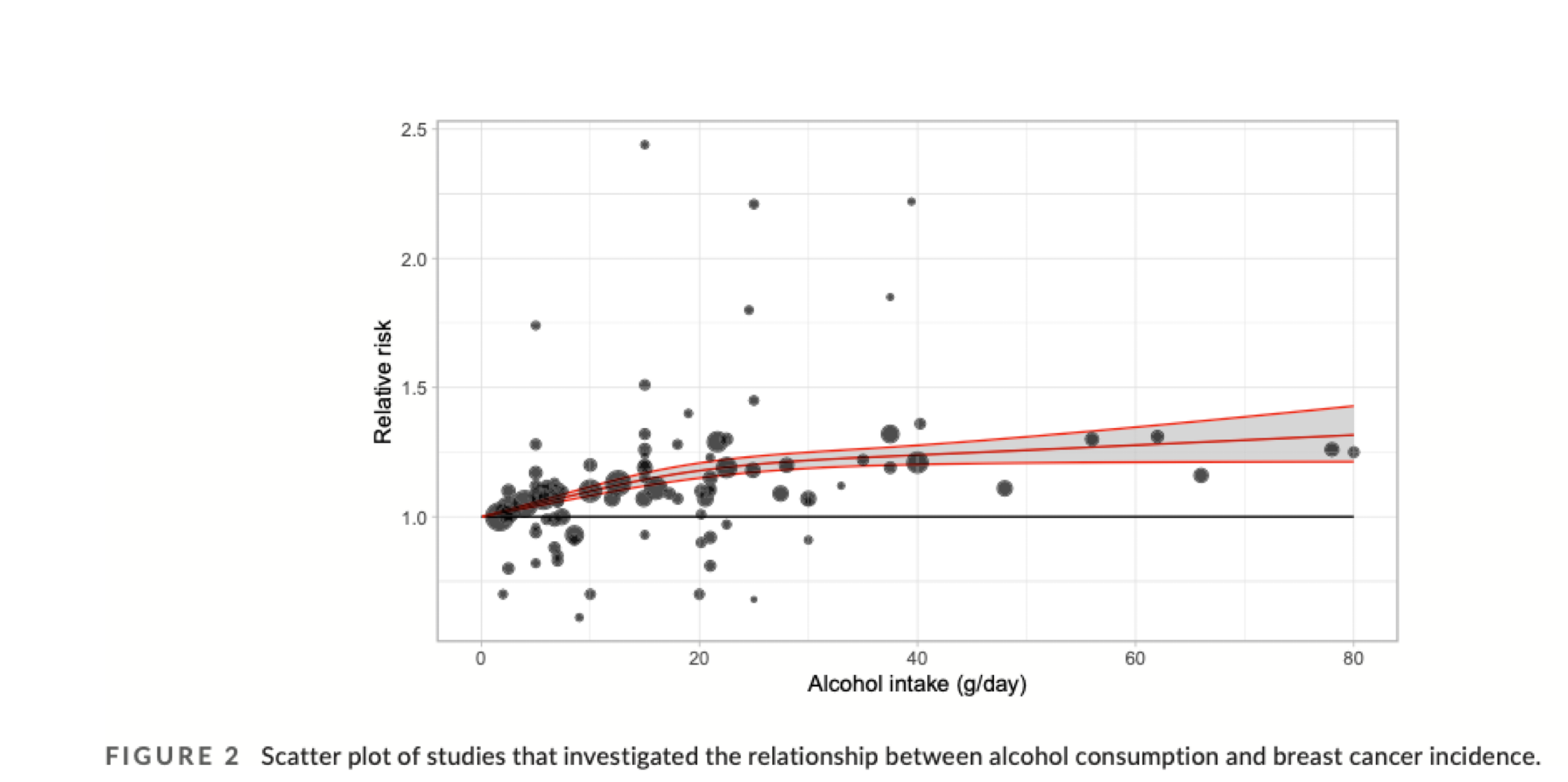
The results are clearly all over the place.
8. Further, some studies have found no association between alcohol consumption and breast cancer risk. For example, Ingold et al. (2019) reported that alcohol increased the risk of head and neck cancers but not breast cancer. A study involving about half a million Britons found no evidence of a causal association between alcohol consumption and breast cancer (Bressaoud et al. 2008). Low and regular consumption of wine reduces the risk of breast cancer (Mourouti et al. 2014). Moderate alcohol consumption, and especially wine consumption, seems to be associated with breast cancer prevention.
9. In 2026, it is no longer sufficient to depend on IARC assessments from 2010 and 2012 based on unknown rationales. It is unacceptable to gloss over results that do not support a position by arguing that the majority of studies show the opposite. A basic principle of the scientific method is that if a study does not support a hypothesis, there must be something wrong with the study or the hypothesis. So which is it?
10. So, for these reasons, I do not support the premise on which this paper is written.”
ISFAR member Kaplan remarks that “this meta-analysis is particularly important because there appears to be broad consensus that alcohol consumption—including light intake—is associated with incident breast cancer and, in some analyses, poorer outcomes. These conclusions have also influenced policy-relevant statements from the WHO, the American Association for Cancer Research, and the U.S. Surgeon General. In addition, concern about breast cancer risk may strongly influence health behaviours among women. With that context, here are a few comments:
1. Overall findings
Some of the core results are not unexpected. The analysis reports an association between alcohol consumption and breast cancer incidence in the overall population, and this association appears consistent across light, moderate, and heavy exposure categories. At the same time, there appears to be a protective association for overall survival, which deserves careful interpretation and discussion.
2. Study exclusions in the PRISMA diagram
All of the critiques were thoughtful, but I was particularly struck by Forum Member Skovenborg’s comments. One point that would benefit from clarification is the exclusion of 22 studies at the third step of the PRISMA diagram (Figure 1). Were these studies excluded because they analysed alcohol exposure and found no statistically significant association with breast cancer (as suggested by Forum Member Skovenborg), or were they excluded because the authors did not report alcohol-related outcomes, perhaps because they were focusing on other associations? Clarifying this distinction would help readers better understand the selection process. If Forum Member Skovenborg’s interpretation is correct (at least the way I read it), there was a serious problem with the inclusion criteria.
3. Number needed to harm
I had hoped to use the reported data to calculate the number needed to harm. Unfortunately, I was unable to locate sufficient information in the manuscript to perform that calculation. Providing absolute risks or additional summary estimates would have been very helpful.”
References
Al-Sader, H., Abdul-Jabar, H., Allawi, Z., & Haba, Y. (2009) Alcohol and breast cancer: the mechanisms explained. J Clin Med Res, 1(3):125-31. doi: 10.4021/jocmr2009.07.1246.
Arecco, L., Cacilhas, P. M., Bobato Lara Gismondi, C., Bruzzone, M., Gentile, G., et al. (2026). Association between alcohol consumption and breast cancer incidence and prognosis: A systematic review and meta-analysis. Breast, 86.
Bessaoud, F., Daurès, J.P. (2008) Patterns of alcohol (especially wine) consumption and breast cancer risk: a case-control study among a population in Southern France. Ann Epidemiol, 18(6):467-75. doi: 10.1016/j.annepidem.2008.02.001.
Brooks, P.J., Zakhari, S. (2013) Moderate alcohol consumption and breast cancer in women: from epidemiology to mechanisms and interventions. Alcohol Clin Exp Res, 37(1):23-30. doi: 10.1111/j.1530-0277.2012.01888.x.
Debela, M. B., Gonfa, K. B., Hussen, M. M., Zenbaba, D., Kahsay, A. B., et al. (2025). Breast cancer determinants in low- to upper-middle-income countries: an umbrella review of meta-analyses of observational studies and an urgent call for implementation science. BMC Cancer, 25(1). https://doi.org/10.1186/s12885-025-14499-w
Francies, F.Z., Hull, R., Khanyile, R., & Dlamini, Z. (2020) Breast cancer in low-middle income countries: abnormality in splicing and lack of targeted treatment options. Am J Cancer Res, 10(5):1568-1591.
Ingold, N., Amin, H.A., & Drenos, F. (2019) Alcohol causes an increased risk of head and neck but not breast cancer in individuals from the UK Biobank study: A Mendelian randomisation analysis, medRxiv, 19002832, 1 – 20. doi: 10.1101/19002832.
Jung, S., Wang, M., Anderson, K., Baglietto, L., Bergkvist, L. et al. (2016) Alcohol consumption and breast cancer risk by estrogen receptor status: in a pooled analysis of 20 studies. Int J Epidemiol, 45(3), 916–928. https://doi.org/10.1093/ije/dyv156
Leitzmann, M. F., Bakogianni, I., Anderson, A. S., Bauld, L., Fernandez, E., et al. (2026). European Code Against Cancer, 5th edition – diet, excess body weight, physical activity, sedentary behaviour, breastfeeding, and cancer. Mol Oncol, 20(1), 28–48. https://doi.org/10.1002/1878-0261.70201
Løyland, B., Sandbekken, I.H., Grov, E.K., & Utne, I. (2024) Causes and risk factors of breast cancer, What do we know for sure? An evidence synthesis of systematic reviews and meta-analyses. Review Cancers (Basel), 16(8):1583.
Kaaks, R., Rinaldi, S., Key, T.J., Berrino, F., Peeters, P.H., et al. (2005a) Postmenopausal serum androgens, oestrogens and breast cancer risk: the European prospective investigation into cancer and nutrition. Endocr Relat Cancer, 12(4):1071-82.
Kaaks, R., Berrino, F., Key, T., Rinaldi, S., Dossus, L. et al. (2005b) Serum sex steroids in premenopausal women and breast cancer risk within the European Prospective Investigation into Cancer and Nutrition (EPIC). J. Natl. Cancer Inst, 97(10):755-65.
Mourouti, N., Kontogianni , M., Papavagelis, C., Psaltopoulou, T., Plytzanopoulou, P., et al. (2014). The J-shaped association between alcohol consumption and breast cancer. Curr Nutr Food Sci, 10(2), 120-127.
Mu, L., & Mukamal, K. J. (2016). Alcohol consumption and rates of cancer screening: Is cancer risk overestimated? Cancer Causes & Control : CCC, 27(2), 281–289. https://doi.org/10.1007/s10552-015-0692-3
Murray, G.J. (2015). Introduction. In: Vasiliou, V., Zakhari, S., Seitz, H., Hoek, J. (eds) Biological Basis of Alcohol-Induced Cancer. Advances in Experimental Medicine and Biology, vol 815. Springer, Cham. https://doi.org/10.1007/978-3-319-09614-8_1
Seitz, H. K., Pelucchi, C., Bagnardi, V., & La Vecchia, C. (2012). Epidemiology and pathophysiology of alcohol and breast cancer: Update 2012. Alcohol Alcohol, 47(3), 204–212. https://doi.org/10.1093/alcalc/ags011
Williams, R.R., & Horm, J.W. (1977) Association of cancer sites with tobacco and alcohol consumption and socioeconomic status of patients interview study from the Third National Cancer Survey. J Nalt Cancer Inst, 58: 525–47.
U.S. Surgeon General. (2025). Alcohol and cancer risk.
Additional readings
Allen, N.E., Beral, V., Casabonne, D., et al. (2009) Moderate Alcohol Intake and Cancer Incidence in Women. J Natl Cancer Inst, 101(5):296–305.
Bagnardi, V., Rota, M., Botteri, E., et al. (2015) Alcohol consumption and site-specific cancer risk: A comprehensive dose–response meta-analysis. Br J Cancer, 112(3):580–593.
IARC Working Group on the Evaluation of Carcinogenic Risks to Humans. Alcohol Consumption and Ethyl Carbamate. IARC Monographs on the Evaluation of Carcinogenic Risks to Humans, Volume 96. Lyon: International Agency for Research on Cancer; 2010.
Shield, K.D., Soerjomataram, I., & Rehm, J. (2016) Alcohol Use and Breast Cancer: A Critical Review. Alcohol Res: Curr Rev, 38(1):15–30.
Smith-Warner, S.A., Spiegelman, D., Yaun, S.S., et al. (1998) Alcohol and Breast Cancer in Women: A Pooled Analysis of Cohort Studies. JAMA, 279(7):535–540.
Comments on this critique by the International Scientific Forum on Alcohol Research were provided by the following members:
Henk Hendriks, PhD, Independent consultant and partner of the Nutrition Consultants Cooperative, Netherlands
Creina Stockley, PhD, MBA, Independent consultant and Adjunct Senior Lecturer in the School of Agriculture, Food and Wine at the University of Adelaide, Australia
Erik Skovenborg, MD, specialized in family medicine, member of the Scandinavian Medical Alcohol Board, Aarhus, Denmark
R. Curtis Ellison, MD, Section of Preventive Medicine/Epidemiology, Boston University School of Medicine, Boston, MA, USA
Raquel Romano, PhD, Independent consultant and Professor of Applied Technology at the University of Aconcagua, Argentina
Richard Harding, PhD, Formerly Head of Consumer Choice, Food Standards and Special Projects Division, Food Standards Agency, UK
Robert M. Kaplan, PhD, Distinguished Professor and faculty member, Stanford School of Medicine Clinical Excellence Research Center, California, USA
Proudly powered by WordPress. Theme by Infigo Software.