Critique 302 – Alcohol Intake and Incidence of Heart Failure and Its Subtypes: VA Million Veteran Program
Nguyen, X.-M.T., Elhouderi, E., Li, Y., Williams, A.R., Gaziano, L., Joseph, J., Gaziano, J.M., Cho, K., Djousse, L. on behalf of the VA Million Veteran Program, Nutrients (2026) 18(3), 471. https://doi.org/10.3390/nu18030471
Abstract
Background: Little is known about the relation between total alcohol intake and beverage types with the risk of heart failure (HF) and its subtypes in the veteran population. This study aims to examine the associations between total and type of alcohol consumption and risk of HF and its subtypes, namely HF with reduced [HFrEF] and preserved [HFpEF] ejection fraction, in a large cohort of US veterans.
Methods: The study cohort included 401,348 Million Veteran Program participants with complete alcohol information collected through a survey and no HF at baseline. HF events were defined as 1 inpatient or 1 outpatient diagnosis code together with at least two ejection fraction (EF) measurements. We defined HFrEF as HF with left ventricular ejection fraction (LVEF) of ≤40% and HFpEF as heart failure with LVEF ≥ 50%. The associations between alcohol intake, type of beverage consumed (i.e., beer, wine, or liquor), and incidence of HF, HFpEF, and HFrEF were assessed using Cox proportional hazard models. Restricted cubic spline regression was used to assess for a dose–response association between alcohol consumption and the risk of HF.
Results: Mean age was 65 years, and 91% were men. With a mean follow-up of 6.4 years, we observed 38,420 incident HF events (15,356 HFrEF, 19,047 HFpEF, and 4017 HF with an EF value of 41–49%). Compared to never drinkers, multivariable adjusted hazard ratios for HF were 0.90 (95% CI: 0.86, 0.94), 0.88 (95% CI: 0.84, 0.93), 0.86 (95% CI: 0.81, 0.91), 0.92 (95% CI: 0.86, 0.98), 0.95 (95% CI: 0.84, 1.06), and 1.08 (95% CI: 1.01, 1.15) for current drinkers of 0.1–0.5, 0.6–1, 1.1–2, 2.1–3, 3.1–4 drinks/day, and heavy drinkers (i.e., >4 drinks/day and/or those diagnosed with alcohol use disorder), respectively. We found a similar association between alcohol intake and risk of HFpEF and HFrEF, except heavy drinking was significantly associated with HFrEF (HR: 1.13, 95% CI: 1.02, 1.24), not HFpEF (HR: 1.05, 95% CI: 0.96, 1.13). Types of alcoholic beverage preference did not influence the alcohol-HF relation.
Conclusions: Our data are consistent with a J-shaped relation between alcohol consumption and risk of heart failure, irrespective of subtypes.
ISFAR Summary
Heart failure (HF) is often caused by conditions that damage the heart muscle. Consequently, the majority of HF patients have multiple comorbidities such as cardiovascular diseases, diabetes, chronic kidney disease, and anaemia.
The study showed that drinking one to two drinks per day was associated with a reduced incidence of HF of about 15%, whereas drinking more than four drinks per day was associated with an increased risk. This association was independent of HF type, various comorbidities, preferred beverage type, drinking history, and other lifestyle factors.
This study was well conducted, as it involved a large population of participants with a high incidence of HF and detailed phenotyping, enabling robust control of relevant confounders. Participants were also classified as never, former, light–moderate, and heavy/AUD consumers, enabling a nuanced assessment of risk.
Unfortunately, the drinking pattern was not characterised. Additionally, participants were mainly older men, which may limit the generalisability of the results. Errors in assessing alcohol consumption and competing risks may also have led to an underestimation of the effects of alcohol intake. The association did not differ by preferred alcoholic beverage, which may suggest that the link is mediated by alcohol itself rather than other compounds in alcoholic beverages.
Background
Heart failure (HF) is a chronic condition in which the heart cannot pump enough blood to meet the body’s needs. This can cause fluid to build up in the lungs, legs, or feet, a condition known as congestive heart failure (Shams et al., 2025).
The incidence of HF in Australia, European countries and the USA ranges widely from 1 to 9 cases per 1000 person-years and depends strongly on the population studied. In developed countries, incidence rates stabilised between 1970 and 1990 and are now thought to be decreasing (Groenewegen et al., 2020). HF causes approximately 1 in 50 deaths in Australia alone[1], where a seemingly higher burden among women could be attributed to the longer life expectancy and higher incidence in later years of life in women than men (Lenzen et al., 2008).
The majority of patients with HF have multimorbidity, and the proportion with three or more chronic comorbidities increased from 68% in 2002 to 87% in 2014 (Conrad et al., 2018). Comorbidity is associated with more severe HF symptoms and is linked to a poor quality of life and a worse prognosis (Van Deursen et al., 2014). Co-morbidities vary, and some report that diabetes, chronic kidney disease, and anaemia are mainly related to heart failure (Van Deursen et al., 2014), while others report a high incidence of cardiovascular co-morbidities (Conrad et al., 2018).
HF is often caused by conditions that damage the heart muscle, such as a heart attack or high blood pressure. Consequently, risk factors for HF include coronary artery disease, high blood pressure, type 2 diabetes and ageing, where it is three or more times higher in the elderly than in the general population. Lifestyle risk factors include smoking, obesity, alcohol or drug abuse and physical inactivity[2].
It may be classified by side of the heart (left vs right), by pumping function, by timing (acute vs chronic), by symptoms limiting physical ability, and by HF stages. Each approach has its pros and cons, and a universal definition and classification of heart failure was proposed, depending on the left ventricular ejection fraction (Bozkurt et al., 2021). Left ventricular ejection fraction (LVEF) was chosen as the primary classification tool for heart failure because it is a powerful prognostic indicator, a direct measure of systolic function, and a crucial determinant for guiding targeted therapies.
Various subtypes of HF are defined by LVEF. These include: HF with preserved ejection fraction (HFpEF) with an LVEF ≥50%; HF with reduced ejection fraction (HFrEF) with an LVEF ≤40%; heart failure with mildly reduced ejection fraction (HFmrEF) with an LVEF of 41% to 49%; and HF with improved ejection fraction (HFimpEF) with an LVEF ≥40% (previously ≤40%) (Heidenreich et al., 2022).
In this interesting paper by Nguyen et al. (2026), HF subtypes HFrEF (r for reduced: an ejection volume of less than 40%) and HFpEF (p for preserved: an ejection volume of more than 50%) were investigated in relation to alcohol consumption. Alcohol consumption was evaluated not only as total alcohol consumption but also subdivided into preference for one of three main beverage types, viz. beer, wine and liquor. These associations were evaluated using the Veterans Affairs Million Veteran Program, a US longitudinal cohort study comprising over a million US veterans.
Critique
This well-conducted study included over 400,000 participants and featured detailed phenotyping, enabling robust control of relevant confounders. Participants were also classified as never, former, light–moderate, and heavy/AUD consumers, enabling a nuanced assessment of risk. They were followed for an average of 6.4 years, during which 38,420 incident HF events were recorded, with similar numbers across the two main subtypes of heart failure, HFrEF and HFpEF. The large number of HF events, evenly distributed across both subtypes, is a notable strength of this study. The overall incidence of HF in this population is relatively high, about 16 per 1000 person-years, compared to the general population, where it ranges from 1 to 9 per 1000 person-years. This figure does not account for the approximately 35,000 prevalent HF cases already excluded from the analysis. How such a high incidence of HF may have influenced the association with alcohol consumption is difficult to determine, but it likely enhanced the reliability of the findings.
Another factor that may have positively influenced the reliability of the association is the similar findings observed for the two subtypes of heart failure. These subtypes do not necessarily indicate two distinct disease aetiologies but rather stages of the same disease with different severity, namely left ventricular ejection fractions of less than 40% and more than 50%.
An important limitation of the study, as the authors mention in the last sentence of their discussion, is the single assessment of alcohol intake at baseline. This might be a real limitation, since people change their behaviour and lifestyle over their lifetimes. However, the average follow-up period was just 6.4 years, suggesting that alcohol consumption was evaluated relatively soon before the outcome measures were assessed.
Another important issue is confounding factors, which are numerous in HF because it coexists with many morbidities. Nguyen et al. (2026) utilise two main models to adjust for these confounding factors; the second model includes all previously mentioned comorbidities, such as diabetes, hypertension, and myocardial infarction. These adjustments are another strength of the study.
The conclusion of a J-shaped relationship between alcohol consumption and HF risk is fully supported by Table 2 and Figure 1, which show the lowest HF risk at 0.6–2 drinks/day and an increased risk for heavy drinkers (HR 1.08).
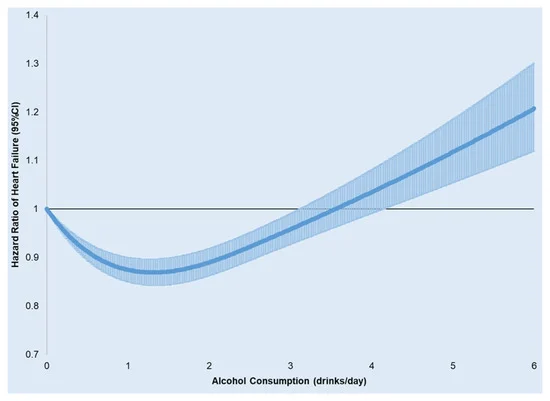
Figure 1. Spline regression of alcohol consumption (drinks/day) and hazard ratios (95% CI) for incident HF. (adjusted for age, gender, race/ethnicity, education level, marital status, income level, exercise frequency, body mass index, DASH score, smoking, statin use, and baseline comorbidities including atrial fibrillation, diabetes, hypercholesterolemia, depression, COPD, stroke, myocardial infarction, and cancers).
All three beverage preferences (and their mixes) were reported to show a similar association with HF and alcohol consumption. Although the analysis was conducted only for total HF and not for the two subtypes, which vary in condition severity, the beneficial effects at moderate drinking levels appear to be mediated by alcohol rather than by other bioactive compounds present in alcoholic beverages. This suggests that muscle function may be improved at moderate levels of alcohol consumption. Although it is clear that heavy drinking and consuming alcohol immediately before exercise negatively affect muscle function, little is known about the effects of habitual moderate alcohol consumption on muscle function. Some studies have shown that adiponectin increases with moderate alcohol consumption, accompanied by increased muscle oxidative capacity (Beulens et al., 2007).
Whereas cardiovascular diseases can result from atherosclerosis, HF results from damage to the heart muscle. This damage may be caused by strenuous conditions affecting the heart muscle, such as hypertension, diabetes, and ageing. Since all these various morbidities often coexist in heart failure, another strength of this study is its correction for these comorbidities and lifestyle factors. However, some potentially relevant factors, such as drinking patterns and stress, may still be omitted. Stress induced by life events like participation in combat may have contributed to the high incidence of heart failure and other comorbidities in this specific population of veterans.
In conclusion, this study ranks among the strongest epidemiological analyses of alcohol consumption and heart failure risk to date, especially for its detailed focus on HF subtypes, large sample size, and high-quality validation of outcomes. The results demonstrating a J-shaped relationship and an increased HFrEF risk among heavy drinkers align with cardiomyopathy physiology and previous meta-analyses. However, it should be noted that the veteran cohort had very limited female representation (approximately 9%), meaning the findings are most relevant to men and should not be broadly generalised to women without further research.
Specific comments
Forum member Ellison regarded this as “an excellent analysis that strongly supports previous research by demonstrating a J-shaped curve in the relationship between alcohol consumption and HF. Notably, it features a large number of subjects with exceptionally high-risk levels for HF, suggesting this may be an ideal cohort for evaluating the link between alcohol and HF. It is observed that among drinkers, the estimated risk for each intake category up to heavy drinking was below 1.00, the risk level for non-drinkers. This may imply that the beneficial effects of alcohol could begin at low consumption levels or that protective results at these levels might stem from under-reporting of intake by subjects.
While the classification of alcohol intake was clearly stated, it is disappointing that the authors lacked data to better classify the “pattern of drinking,” particularly whether beverages were consumed regularly and with food. Such information might have revealed greater effects among drinkers who consumed alcohol, especially wine, daily and with food—the traditional pattern seen in southern Europe, where wine is considered part of daily meals.
The medical and socioeconomic factors known to influence the relationship between alcohol and disease, such as education and income, were appropriately included as potential confounders. Another strength of the paper is the authors’ approach of combining drinkers who report light drinking but show evidence of alcohol misuse, such as alcoholic liver disease or hospitalisations due to ‘alcoholism’, with those who self-report heavy drinking. In other words, it is crucial to include individuals with evidence of alcohol use disorders within the ‘heavy drinking’ categories, regardless of their current self-reported level of alcohol consumption. This was clearly demonstrated by Klatsky et al. (1981, 1983), who reported that indicators of abuse aided in classifying such individuals as current or former ‘heavy drinkers’. Regardless of what they now report as their intake, these individuals should not be grouped with true ‘light drinkers’ (those with no other data indicating alcohol misuse) when assessing the effects of alcohol.”
Forum member Romano notes that this study “analyses the relationship between alcohol consumption and the risk of developing AF, one of the most common cardiac arrhythmias and a condition with significant clinical consequences, addressing alcohol as a potentially modifiable risk factor. The research is based on observational data collected from a large cohort of patients receiving care within the US Department of Veterans Affairs healthcare system, primarily comprising war veterans. This design provides a substantial sample size and enables the evaluation of associations between exposure (alcohol consumption) and outcome (AF) in a real-world clinical setting.
Several methodological limitations should be recognised. The study treats AF as a relatively uniform outcome, without clearly distinguishing among clinical subtypes. Additionally, alcohol consumption is assessed via self-report, which may introduce recall bias or underreporting. Moreover, since the sample mainly comprises veterans, most of whom are men, the applicability of the findings to broader populations is limited. Over an average follow-up of 6.4 years, a significant number of HF events were recorded, totalling 38,420 cases, providing substantial statistical power to detect associations.
While observing a J-shaped relationship between alcohol consumption and the risk of HF suggests that low to moderate intake (around 0.6–2 drinks per day) is associated with the lowest relative risk, such patterns should be interpreted with caution, as observational studies may be affected by residual confounding or differences in baseline health status among groups, including the well-known “healthy drinker” effect. Furthermore, the finding that heavy alcohol consumption (>4 drinks per day) is associated with a higher risk of HFrEF but not HFpEF is physiologically plausible, since excessive alcohol intake can cause direct toxic effects on the myocardium and lead to systolic dysfunction. However, the significant predominance of male participants and the observational nature of the study limit the wider applicability of the results and prevent establishing a definitive causal link between alcohol consumption and the different types of heart failure.
Overall, this study offers important epidemiological evidence about the potential role of alcohol consumption as a risk factor for HF. However, the findings should be viewed cautiously because of the inherent limitations of observational study designs and the specific characteristics of the study population.”
Forum member Waterhouse considers that “overall, this appears to be a substantive study as noted above. I am not surprised by the high incidence of HF compared to the general population, as the average age of the study group was 65 years. As with many other studies, this one is also limited by the lack of data on drinking pattern.”
Forum member McIntosh comments that “this study investigates the effect of alcohol consumption on HF outcomes using a large US sample of predominantly male veterans. The primary findings are presented in Table 2, which shows that hazard ratios in the unadjusted models have a J shape, a pattern observed by many other researchers: all forms of alcohol consumption have beneficial effects on longevity, contrary to claims made by some of the New Temperance researchers, such as Zhao et al. (2023), in their examination of the relationship between alcohol use and all-cause mortality.
The unadjusted models show the largest effects. Hazard ratios are smaller in this case because they account for the total impact of alcohol use over the lifetime. In adjusted models, some of the effect of alcohol use is attributed to regressors like education or income, which are correlated with alcohol use, and therefore these estimates underestimate the true effects of alcohol on life durations.
There are two potential biases in the results. The first is competing risk bias. As shown in McIntosh (2014), failing to account for the censoring of heart disease durations and other causes of death like cancer can lead to biased estimates of the effect of alcohol on heart failure durations. The direction of this bias depends on how alcohol use affects cancer mortality.
If cancer patients are alcohol consumers it is commonly believed that they will live less long than non-users. But the effect on heart failure durations will be shorter durations because of the censuring of these by cancer deaths. Thus, the estimated effects of alcohol consumption on HF durations are likely underestimated. This aligns with the findings in Mewton et al. (2023: Table 3), who observed larger effects in competing risk models.
The second bias arises from possible measurement errors in the amount of alcohol consumed. There are valid concerns here, as significant discrepancies exist between survey self-reported consumption and actual alcohol sales data. However, simulations using American BRFSS data on heart disease for 2023 showed that, although plausible increases in alcohol consumption decreased the effect on the likelihood of developing heart disease, the significant J-shaped relationship identified by the authors of this paper remained.
In conclusion, this is an important new contribution to the long and sometimes contentious literature on the benefits of alcohol use. I can find no credible reason to doubt their results.“
Forum member Harding “endorses the comments of others regarding the lack of data on drinking patterns within this very large cohort. I only have a couple of additional points. The first is that the cohort consisted of 91% men. It might have been better to make the cohort 100% men, as that would have eliminated one variable. One of the earlier papers on this subject (Arafa et al., 2023) found a J-shaped relationship among Japanese men, but not among women, so that would have enabled a direct comparison with that study.
Secondly, the authors defined beverage preference as whether or not a single beverage contributed to more than 50% of the total alcohol consumed, based on food frequency questionnaires. That does not seem to me a very clear distinction and, therefore, makes it difficult to draw any definitive conclusions. Another earlier study (Yeo et al., 2022) concerned a cohort from a population-based study in Korea, and indeed, the association was J-shaped. An earlier ISFAR critique (#295) revealed that almost all alcohol consumption in Korea was from soju, a grain-based spirit with about 20% alcohol, so it was presumably also mainly consumed by those in the Yeo cohort study.”
References
Arafa, A., Kashima, R., Kokubo, Y., Teramoto, M., Sakai, Y., Nosaka, S., Kawachi, H., Shimamoto, K., Matsumoto, C., Gao, Q., & Izumi, C. (2023) Alcohol consumption and the risk of heart failure: the Suita Study and meta-analysis of prospective cohort studies.Environmental Health and Preventative Medicine, 28, 26. https://doi.org/10.1265/ehpm.22-00231.
Beulens, J. W. J., Van Loon, L. J. C., Kok, F. J., Pelsers, M., Bobbert, T., Spranger, J., Helander, A., & Hendriks, H. F. J. (2007). The effect of moderate alcohol consumption on adiponectin oligomers and muscle oxidative capacity: a human intervention study. Diabetologia, 50(7), 1388–1392. https://doi.org/10.1007/s00125-007-0699-8
Bozkurt, B., Coats, A. J. S., Tsutsui, H., Abdelhamid, C. M., Adamopoulos, S., Albert, N., Anker, S. et al. (2021). Universal definition and classification of heart failure: a report of the Heart Failure Society of America, Heart Failure Association of the European Society of Cardiology, Japanese Heart Failure Society and Writing Committee of the Universal Definition …. European Journal of Heart Failure, 23(3), 352–380. https://doi.org/10.1002/ejhf.2115
Conrad, N., Judge, A., Tran, J., Mohseni, H., Hedgecott, D., Crespillo, A. P., Allison, M., Hemingway, H., Cleland, J. G., McMurray, J. J. V., & Rahimi, K. (2018). Temporal trends and patterns in heart failure incidence: a population-based study of 4 million individuals. The Lancet, 391(10120), 572–580. https://doi.org/10.1016/S0140-6736(17)32520-5
Groenewegen, A., Rutten, F. H., Mosterd, A., & Hoes, A. W. (2020). Epidemiology of heart failure. European Journal of Heart Failure, 22(8), 1342–1356. https://doi.org/10.1002/ejhf.1858
Heidenreich, P. A., Bozkurt, B., Aguilar, D., Allen, L. A., Byun, J. J., Colvin, M. M., Deswal, A. et al. (2022). 2022 AHA/ACC/HFSA Guideline for the Management of Heart Failure: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation, 145(18), E895–E1032. https://doi.org/10.1161/CIR.0000000000001063.
Klatsky, A. L., Friedman, G. D., & Siegelaub, A. B. (1981). Alcohol and mortality. A ten-year Kaiser-Permanente experience. Annals of Internal Medicine, 95(2), 139–145.
Klatsky, A. L., Armstrong, M. A., & Friedman, G. D. (1983). Racial patterns of alcoholic beverage use. Alcoholism: Clinical and Experimental Research, 7(2), 172-177
Lenzen, M.J., Rosengren, A., Scholte, O.P., Reimer, W.J., Follath, F., Boersma, E., Simoons, M.L., Cleland, J.G., & Komajda, M. (2008) Management of patients with heart failure in clinical practice: differences between men and women. Heart, 94(3):e10. https://doi.org/10.1136/hrt.2006.099523.
Mcintosh, J. (2024) Inference problems in the analysis of the relationship between alcohol consumption and coronary heart disease. Communications in Statistics-Simulation and Computation, 43(10), 2275-2282.
Mewton, L., Visontay, R., Hoy, N., Lipnicki, D.M., Sunderland, M., Lipton, R.B., Guerchet, M, et al. & Collaborators from the Cohort Studies of Memory in an International Consortium (COSMIC). (2023) The relationship between alcohol use and dementia in adults aged more than 60 years: a combined analysis of prospective, individual-participant data from 15 international studies. Addiction. 2023 Mar;118(3):412-424. https://doi.org/10.1111/add.16035. Erratum in: Addiction. 2024 Oct;119(10):1848. https://doi.org/10.1111/add.16512.
Nguyen, X. M. T., Elhouderi, E., Li, Y., Williams, A. R., Gaziano, L., Joseph, J., Gaziano, J. M., Cho, K., & Djousse, L. (2026). Alcohol Intake and Incidence of Heart Failure and Its Subtypes: VA Million Veteran Program. Nutrients, 18(3). https://doi.org/10.3390/nu18030471
Shams, P., Malik, A., & Chhabra, L. (2025) Heart Failure (Congestive Heart Failure) [Updated 2025 Feb 26]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025 Jan-. Available from: https://www.ncbi.nlm.nih.gov/books/NBK430873/
Van Deursen, V. M., Urso, R., Laroche, C., Damman, K., Dahlström, U., Tavazzi, L., Maggioni, A. P., & Voors, A. A. (2014). Co-morbidities in patients with heart failure: an analysis of the European Heart Failure Pilot Survey. European Journal of Heart Failure, 16(1), 103–111. https://doi.org/10.1002/ejhf.30
Yeo, Y., Jeong, S.M., Shin, D.W., Han, K., Yoo, J., Yoo, J.E., & Lee, S.P. (2022) Changes in alcohol consumption and risk of heart failure: A nationwide population-based study in Korea. International Journal of Environmental Research and Public Health, 19(23),16265. https://doi.org/10.3390/ijerph192316265.
Zhao, J., Stockwell, T., Naimi, T., Churchill, S., Clay, J., & Sherk, A. (2023). Association between daily alcohol intake and risk of all-cause mortality: a systematic review and meta-analyses. JAMA Network Open, 6(3), e236185-e236185.
Comments on this critique by the International Scientific Forum on Alcohol Research were provided by the following members:
Henk Hendriks, PhD, Independent consultant and partner of the Nutrition Consultants Cooperative, Netherlands
Creina Stockley, PhD, MBA, Independent consultant and Adjunct Senior Lecturer in the School of Agriculture, Food and Wine at the University of Adelaide, Australia
R. Curtis Ellison, MD, Section of Preventive Medicine/Epidemiology, Boston University School of Medicine, Boston, MA, USA
Raquel Romano, PhD, Independent consultant and Professor of Applied Technology at the University of Aconcagua, Argentina
Andrew L. Waterhouse, PhD, Professor Emeritus of Enology, Department of Viticulture and Enology, University of California, Davis, CA, USA
James McIntosh, PhD, Retired Professor of Economics, Concordia University, Montreal, Canada
Richard Harding, PhD, Formerly Head of Consumer Choice, Food Standards and Special Projects Division, Food Standards Agency, UK
[1] AIHW: Field B. Heart failure…what of the future? Bulletin no. 6. AIHW Cat. No. AUS 34. Canberra: AIHW; 2003.
[2] https://www.heart.org/en/health-topics/heart-failure/causes-and-risks-for-heart-failure#:~:text=heart%20failure%20include:-,Smoking,Not%20being%20physically%20active
Proudly powered by WordPress. Theme by Infigo Software.